Accelerated Peer-to-Peer (AP2P)
Our Accelerated Peer-to-Peer (AP2P) methodology bypasses traditional administrative bottlenecks by deploying a board-certified sub-specialist within six hours of a denial trigger. By matching the Payor’s medical director rank-for-rank, we immediately elevate the conversation from a generalized administrative review to a rigorous clinical discussion. This proactive intervention promotes real-time engagement with the patient’s evolving acuity before administrative “denial drift” can take hold.
Explore All Services →
How We Support Our Clients
Our approach relies on a comprehensive, multi-step process integrated directly into hospital workflows.
Upon receiving a denial trigger, we perform a 3-minute clinical scrub of the EMR to prevent the case from stalling in the appeals queue.
We activate a rank-matched physician (e.g., matching a cardiology denial with a board-certified cardiologist) to ensure specialty parity, creating a “Deference Factor” that makes generalist Payor directors structurally hesitant to overrule our specialist’s technical nuances.
Prior to the call, our specialist conducts a 60-minute deep chart dive, mapping objective clinical data — such as SOFA scores, lactate trends, and Two-Midnight benchmarks — into an AI-assisted Tactical Prep Sheet verified by a Nurse Auditor.
During the live Peer-to-Peer, our specialist bypasses generalized criteria to focus on established guidelines like ACC/AHA or NCCN. Every word is documented as a Certified Arbitrator’s Record to build a litigation-ready evidentiary file; if the denial is upheld, we immediately file a Sentinel Dispute to escalate to the Federal IDR track.
Accelerated Peer-to-Peer (AP2P)
In 2026, where Payor AI can issue a denial in milliseconds, the standard P2P has become a bottleneck. Our Accelerated P2P deploys a board-certified sub-specialist within 6 hours, matching the Payor medical director rank-for-rank and converting the conversation from administrative to clinical — and are designed to achieve 65–80% appeal overturn rates.

The primary value of a P2P within six hours is immediate preservation of the Clinical Narrative before it is diluted by administrative processing. By intervening at this stage, we force the Payor Medical Director to engage with a living patient’s evolving acuity — not a static retrospective chart.
- 3-Minute Clinical Scrub of EMR upon denial trigger
- Prevents 'denial drift' before the case enters the appeals queue
- Forces real-time engagement over retrospective paper review
- Protects Length of Stay efficiency by resolving status disputes on Day 1

Our Specialist is matched to a Payor Medical Director of equivalent clinical standing. A Cardiology denial triggers a Cardiovascular Specialist. A Payor’s Generalist Medical Director is structurally hesitant to overrule a Board-Certified Sub-Specialist on technical nuances — creating the Deference Factor.
- 40–50% increase in overturn rates vs. generalist-led P2Ps
- Specialist-to-specialist calls resolved in 8–10 min vs. 30 min standard
- Bypasses the educational phase — straight to ACC/AHA or NCCN guidelines
- Identifies Criteria Drift in real-time during the call
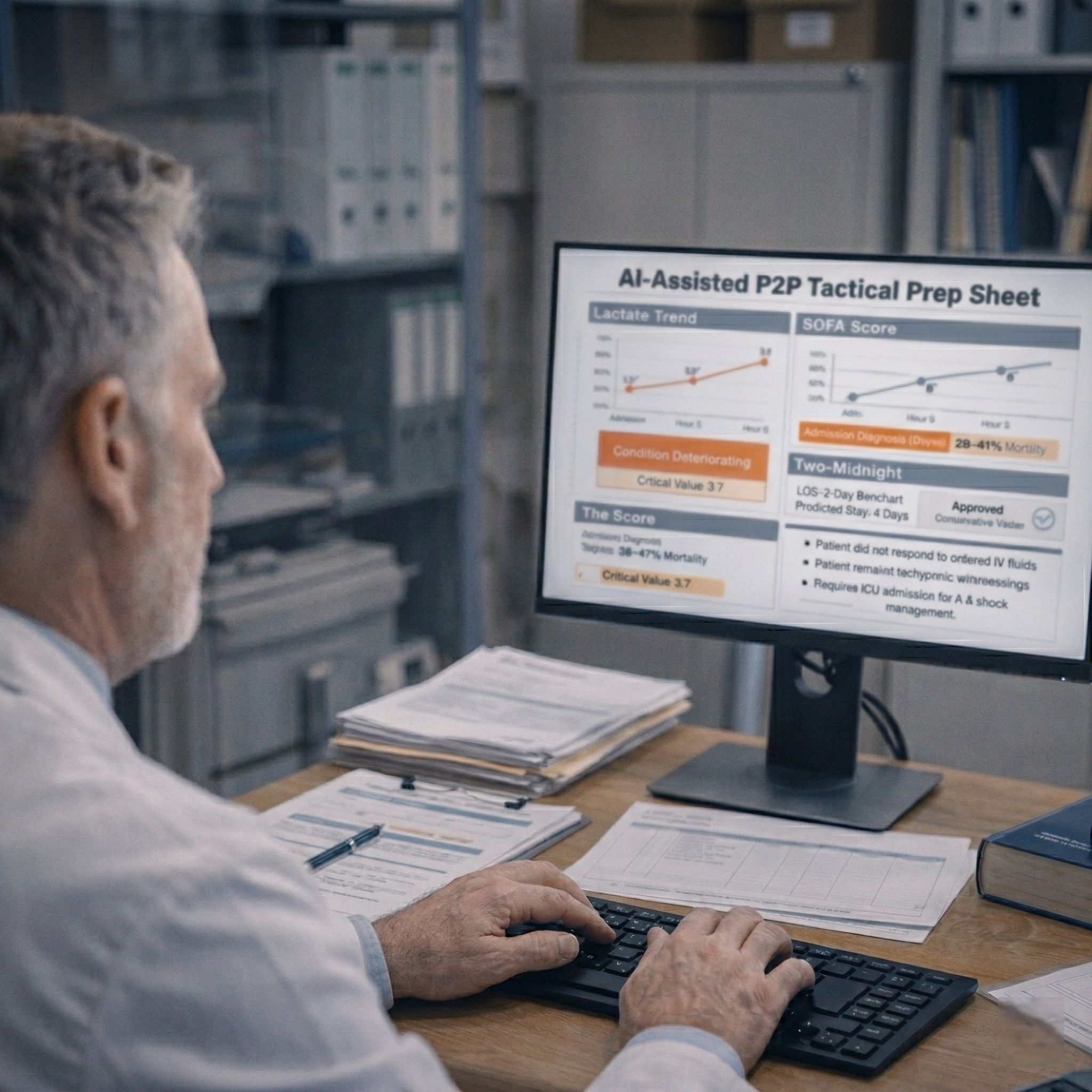
While a hospital physician has 5–10 minutes to prepare between rounds, our Specialist receives a 60-minute deep chart dive before the call — mapping lactate trends, SOFA scores, Two-Midnight benchmarks, and ‘failed conservative management’ data points into an AI-assisted P2P Tactical Prep Sheet.
- 60-minute forensic chart review vs. 5-min hospital standard
- Maps SOFA scores, lactate trends, and objective clinical data
- AI-assisted Tactical Prep Sheet verified by a Nurse Auditor
- Builds litigation-ready evidentiary record before the call begins

Payors are substantially less likely to issue bad-faith denials when they know an independent firm is documenting every word for potential IDR or legal escalation. If the denial is upheld, we file a Sentinel Dispute and escalate immediately to the Federal IDR track under the No Surprises Act.
- Every P2P word documented as a Certified Arbitrator’s Record
- Regulatory Non-Compliance flag issued when Criteria Drift is identified
- Sentinel Dispute filed if denial is upheld — No Surprises Act IDR track
- Operational deterrent: friction cost of defending denial exceeds Payor savings

Behind every denial is a patient whose care, coverage, and financial stability are directly impacted. MHMDAA’s Accelerated Peer-to-Peer (AP2P) process safeguards patients from the consequences of inappropriate or premature status determinations by ensuring that clinical decisions are rendered by qualified physicians based on real-time acuity and objective clinical data—not automated systems applying generalized criteria. By preserving appropriate inpatient status at the point of review, patients maintain uninterrupted access to medically necessary services. When a denial is reversed within 6 hours, there is no gap in care, no delay in treatment, and no unexpected out-of-pocket liability.
- Prevents inappropriate downgrades from Inpatient to Observation
- Reduces risk of surprise billing and unexpected out-of-pocket expense for patients
- Preserves continuity of medically necessary treatment without administrative interruption
- Maintains accurate representation of patient acuity, ensuring that the patient’s clinical presentation and course are not overshadowed by rigid or generalized decision logic.
Start The Conversation With Our Experts
Partner with MHMDAA's physician-led team and take the first decisive step toward building a denial-resilient, financially sustainable hospital operation.